Vegans, Vegetarians and Pescatarians Are at Risk of Iodine Deficiency in Norway

 ,
,  , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
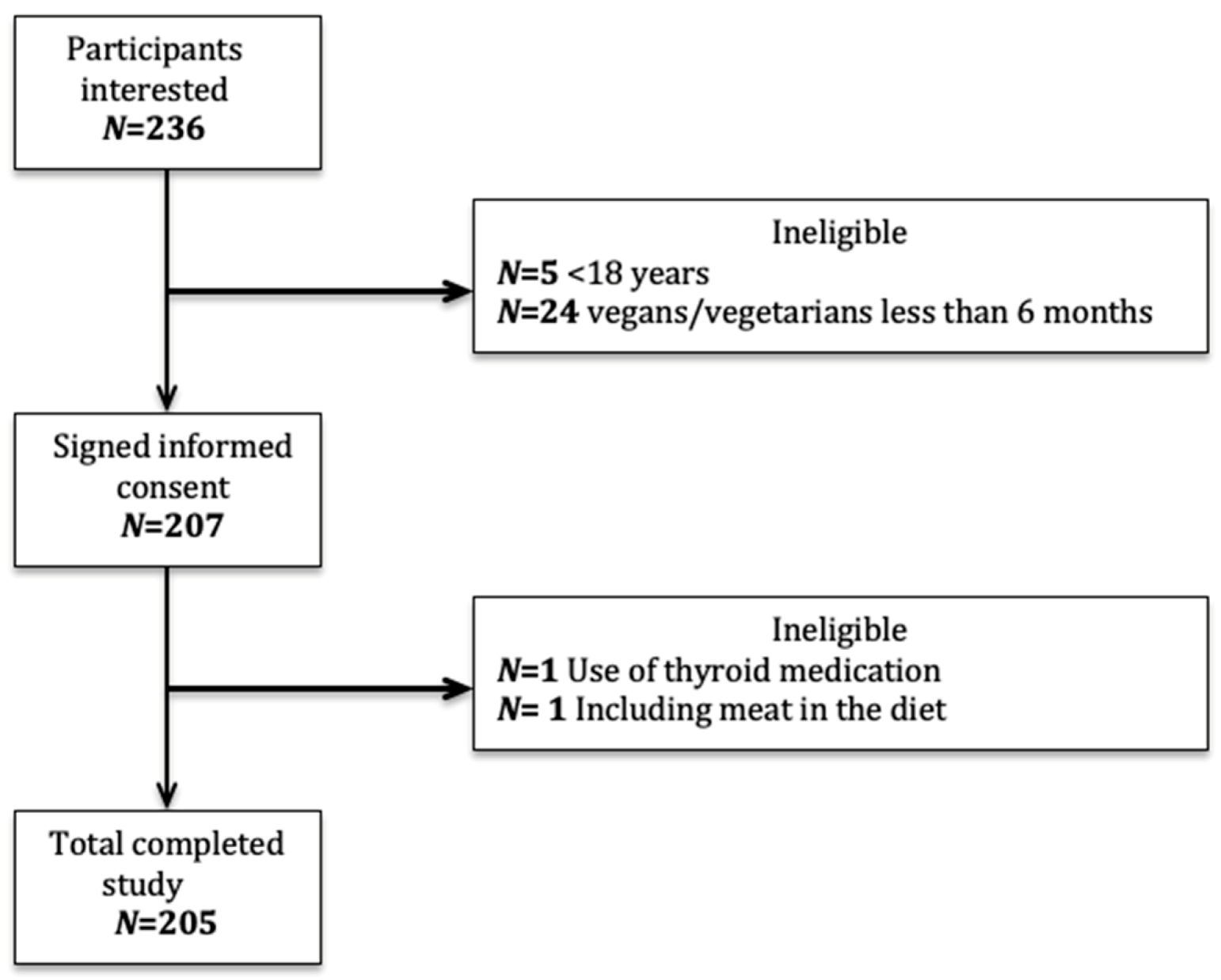
2.1. Subjects
2.2. Study Participation
2.3. Determination of Urinary Iodine Concentration
2.4. Assessment and Calculation of Iodine Intake from Foods
2.5. Assessment and Calculation of Iodine Intake from Supplements and Macroalgae
2.6. Calculation of Iodine Knowledge Score
2.7. Ethical Approval
2.8. Definitions of Iodine Status and Recommended Iodine Intake
2.9. Statistics
3. Results
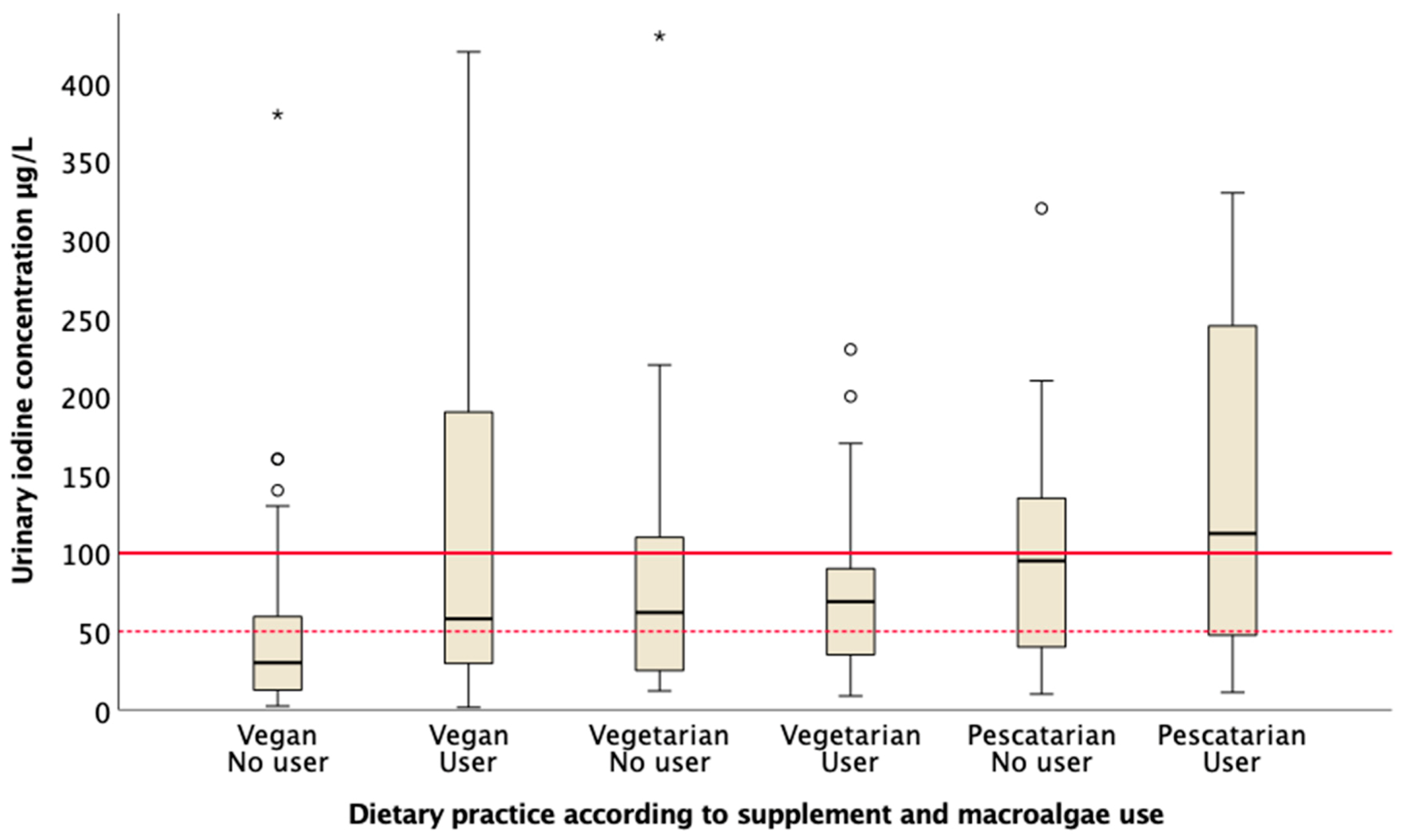
3.1. Urinary Iodine Concentration

3.2. Dietary Intake of Iodine from Food and Supplements
3.3. Iodine Knowledge Score and Associations with UIC and Iodine Intake
3.4. Predictors for Urinary Iodine Concentration
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Leitzmann, C. Vegetarian nutrition: Past, present, future. Am. J. Clin. Nutr. 2014, 100, 496–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bugge, A.B.A. Meatless Eating Habits—Consumers Views; SIFO: Oslo, Norway, 2018; p. 83. ISBN 82-7063-480-8. [Google Scholar]
- The Danish Vegan Society. Facts About Plant-Based Living in Denmark. 2019. Available online: https://vegetarisk.dk/aboutus/ (accessed on 5 July 2020).
- The Swedish Animal Rights. Every Tenth Swede is Vegan. 2014. Available online: https://www.djurensratt.se/blogg/var-tionde-svensk-ar-vegetarian (accessed on 5 July 2020).
- Craig, W.J. Health effects of vegan diets. Am. J. Clin. Nutr. 2009, 89, 1627S–1633S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schüpbach, R.; Wegmüller, R.; Berguerand, C.; Bui, M.; Herter-Aeberli, I. Micronutrient status and intake in omnivores, vegetarians and vegans in Switzerland. Eur. J. Nutr. 2015, 56, 283–293. [Google Scholar] [CrossRef] [PubMed]
- Elorinne, A.L.; Alfthan, G.; Erlund, I.; Kivimaki, H.; Paju, A.; Salminen, I.; Turpeinen, U.; Voutilainen, S.; Laakso, J. Food and Nutrient Intake and Nutritional Status of Finnish Vegans and Non-Vegetarians. PLoS ONE 2016, 11, e0148235. [Google Scholar] [CrossRef] [Green Version]
- Dahl, L.; Opsahl, J.A.; Meltzer, H.M.; Julshamn, K. Iodine concentration in Norwegian milk and dairy products. Br. J. Nutr. 2003, 90, 679–685. [Google Scholar] [CrossRef]
- Carlsen, M.H.; Andersen, L.F.; Dahl, L.; Norberg, N.; Hjartaker, A. New Iodine Food Composition Database and Updated Calculations of Iodine Intake among Norwegians. Nutrients 2018, 10, 930. [Google Scholar] [CrossRef] [Green Version]
- Nerhus, I.; Markhus, M.W.; Nilsen, B.M.; Øyen, J.; Maage, A.; Ødegård, E.R.; Kjellevold, M. Iodine content of six fish species, Norwegian dairy products and Hen’s egg. Food Nutr. Res. 2018, 62. [Google Scholar] [CrossRef] [Green Version]
- Zimmermann, M.B. The role of iodine in human growth and development. Semin. Cell Dev. Biol. 2011, 22, 645–652. [Google Scholar] [CrossRef]
- Lazarus, J.H. Iodine Status in Europe in 2014. Eur. Thyroid J. 2014, 3, 3–6. [Google Scholar] [CrossRef] [Green Version]
- Henjum, S.; Abel, M.H.; Meltzer, H.M.; Dahl, L.; Alexander, J.; Torheim, L.E.; Brantsæter, A.L. Is iodine intake adequate in Norway? Tidsskr. Nor. Legeforeningen 2019, 139. [Google Scholar] [CrossRef]
- Hynes, K.L.S.; Otahal, P.; Oddy, W.H.; Burgess, J.R. Women Remain at Risk of Iodine Deficiency during Pregnancy: The Importance of Iodine Supplementation before Conception and Throughout Gestation. Nutrients 2019, 11, 172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panth, P.; Guerin, G.; DiMarco, N.M. A Review of Iodine Status of Women of Reproductive Age in the USA. Biol. Trace Elem. Res. 2019, 188, 208–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krajcovicová-Kudlácková, M.; Buckovà, K.; Klimes, I.; Sebokovà, E. Iodine deficiency in vegetarians and vegans. Ann. Nutr. Metab. 2003, 47, 183–185. [Google Scholar] [CrossRef] [PubMed]
- Lightowler, H.J.; Daive, G.J. Iodine intake and iodine deficiency in vegans as assesses by duplicate-portion technique and urinary iodine excretion. Br. J. Nutr. 1998, 80, 529–535. [Google Scholar] [CrossRef] [Green Version]
- Fallon, N.; Dillon, S.A. Low Intakes of Iodine and Selenium Amongst Vegan and Vegetarian Women Highlight a Potential Nutritional Vulnerability. Front Nutr. 2020, 7, 72. [Google Scholar] [CrossRef]
- Brantsaeter, A.L.; Knutsen, H.K.; Johansen, N.C.; Nyheim, K.A.; Erlund, I.; Meltzer, H.M.; Henjum, S. Inadequate Iodine Intake in Population Groups Defined by Age, Life Stage and Vegetarian Dietary Practice in a Norwegian Convenience Sample. Nutrients 2018, 10, 230. [Google Scholar] [CrossRef] [Green Version]
- Leung, A.M.; Lamar, A.; He, X.; Braverman, L.E.; Pearce, E.N. Iodine status and thyroid function of Boston-area vegetarians and vegans. J. Clin. Endocrinol. Metab. 2011, 96, 1303–1307. [Google Scholar] [CrossRef] [Green Version]
- Henjum, S.; Brantsæter, A.L.; Kurniasari, A.; Dahl Aadland, E.K.; Gjengedal, E.L.F.; Aakre, I. Suboptimal iodine Status and Low Iodine Knowledge in young Norwegian women. Nutrients 2018, 10, 941. [Google Scholar] [CrossRef] [Green Version]
- Duinker, A.; Roiha, I.S.; Amlund, H.; Dahl, L.; Lock, E.-J.; Kögel, T.; Lunestad, T. Potential Risks Posed by Macro Algae for Application as Fees and Food—A Norwegian Perspective; National Institute and Seafood Research (NIFES): Bergen, Norway, 2016.
- Eveleigh, E.R.; Coneyworth, L.J.; Avery, A.; Welham, S.J.M. Vegans, Vegetarians, and Omnivores: How Does Dietary Choice Influence Iodine Intake? A Systematic Review. Nutrients 2020, 12, 1606. [Google Scholar] [CrossRef]
- The Norwegian Food Composition Table. The Norwegian Food Safety Authority. 2019. Available online: www.matvaretabellen.no (accessed on 7 November 2019).
- Roleda, M.Y.; Skjermo, J.; Marfaing, H.; Jónsdóttir, R.; Rebours, C.; Gietl, A.; Nitschke, U. Iodine content in bulk biomass of wild-harvested and cultivated edible seaweeds: Inherent variations determine species-specific daily allowable consumption. Food Chem. 2018, 254, 333–339. [Google Scholar] [CrossRef]
- Van Netten, C.; Hoption Cann, S.A.; Morley, D.R.; Van Netten, J.P. Elemental and radioactive analysis of commercially available seaweed. Sci. Total Environ. 2000, 255, 169–175. [Google Scholar] [CrossRef]
- Garnweidner-Holme, L.; Aakre, I.; Lilleengen, A.M.; Brantsaeter, A.L.; Henjum, S. Knowledge about Iodine in Pregnant and Lactating Women in the Oslo Area, Norway. Nutrients 2017, 9, 493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Assessment of Iodine Deficiency Disorders and Monitoring Their Elimination: A Guide for Programme Managers. World Health Organization. UNICEF. ICCIDD. 2007. Available online: http://www.who.int/nutrition/publications/micronutrients/iodine_deficiency/9789241595827/en/ (accessed on 6 June 2018).
- Food and Nutrition Board, Institute of Medicine. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; National Academies Press: Washington, DC, USA, 2001.
- Nordic Nutrition Recommendations. Integrating Nutrition and Physcical Activity, 5th ed.; Nordic Council of Ministers: Copenhagen, Denmark, 2012.
- Lindsay, H.; Allen, A.L.C.; Suzanne, P. Murphy, Perspective: Proposed Harmonized Nutrient Reference Values for Populations. Adv. Nutr. 2020, 11, 469–483. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associate: New York, NY, USA, 1988. [Google Scholar]
- The Norwegian Directorate of Health. Vegetarian and Vegan Diet—Nutritional Plant-Based Diet. 2020. Available online: https://helsenorge.no/kosthold-og-ernaring/vegetarisk-kosthold/naringsrik-vegetarkost (accessed on 9 September 2020).
- Kristensen, N.B.; Madsen, M.L.; Hansen, T.H.; Allin, K.H.; Hoppe, C.; Fagt, S.; Pedersen, O. Intake of macro- and micronutrients in Danish vegans. Nutr. J. 2015, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abel, M.H.; Ystrom, E.; Caspersen, I.H.; Meltzer, H.M.; Aase, H.; Torheim, L.E.; Askeland, R.B.; Reichborn-Kjennerud, T.; Brantsaeter, A.L. Maternal Iodine Intake and Offspring Attention-Deficit/Hyperactivity Disorder: Results from a Large Prospective Cohort Study. Nutrients 2017, 9, 1239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abel, M.H.; Korevaar, T.I.M.; Erlund, I.; Villanger, G.D.; Caspersen, I.H.; Arohonka, P.; Alexander, J.; Meltzer, H.M.; Brantsaeter, A.L. Iodine Intake is Associated with Thyroid Function in Mild to Moderately Iodine Deficient Pregnant Women. Thyroid 2018, 28, 1359–1371. [Google Scholar] [CrossRef]
- Abel, M.H.; Brandlistuen, R.E.; Caspersen, I.H.; Aase, H.; Torheim, L.E.; Meltzer, H.M.; Brantsaeter, A.L. Language delay and poorer school performance in children of mothers with inadequate iodine intake in pregnancy: Results from follow-up at 8 years in the Norwegian Mother and Child Cohort Study. Eur. J. Nutr. 2019, 58, 3047–3058. [Google Scholar] [CrossRef] [Green Version]
- Markhus, M.W.; Dahl, L.; Moe, V.; Abel, M.H.; Brantsæter, A.L.; Øyen, J.; Kjellevold, M. Maternal Iodine Status is Associated with Offspring Language Skills in Infancy and Toddlerhood. Nutrients 2018, 10, 1270. [Google Scholar] [CrossRef] [Green Version]
- Moe, V.; Fredriksen, E.; Kjellevold, M.; Dahl, L.; Markhus, M.W.; Stormark, K.M.; Soest, T.V.; Smith, L. Little in Norway: A prospective longitudinal community-based cohort from pregnancy to child age 18 months. BMJ Open 2019, 9, 12. [Google Scholar] [CrossRef] [Green Version]
- Zhao, W.; Li, X.; Xia, X.; Gao, Z.; Han, C. Iodine Nutrition During Pregnancy: Past, Present, and Future. Biol. Trace Elem. Res. 2018, 188, 196–207. [Google Scholar] [CrossRef]
- Laurberg, P.; Jorgensen, T.; Perrild, H.; Ovesen, L.; Knudsen, N.; Pedersen, I.B.; Rasmussen, L.B.; Carle, A.; Vejbjerg, P. The Danish investigation on iodine intake and thyroid disease, DanThyr: Status and perspectives. Eur. J. Endocrinol. 2006, 155, 219–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Groufh-Jacobsen, S.; Mosand, L.M.; Bakken, K.S.; Solvik, B.S.; Oma, I.; Gjengedal, E.L.F.; Brantsaeter, A.L.; Strand, T.A.; Henjum, S. Mild to Moderate Iodine Deficiency and Inadequate Iodine Intake in Lactating Women in the Inland Area of Norway. Nutrients 2020, 12, 630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Combet, E.; Ma, Z.F.; Cousins, F.; Thompsons, B.; Lean, M.E.J. Low-level seaweed supplementation improved iodine status in iodine-insufficient women. Br. J. Nutr. 2014, 112, 753–761. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
| Vegans a | Vegetarians a | Pescatarians a | Total | |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | |
| Participants | 115 | 55 | 35 | 205 |
| Gender | ||||
| Females | 74 (64) | 43 (78) | 31 (89) | 148 (72) |
| Males | 41 (36) | 12 (22) | 4 (11) | 57 (28) |
| Planning pregnancy, (2 years period) | ||||
| Yes | 14 (19) | 5 (12) | 6 (19) | 25 (17) |
| No | 58 (78) | 38 (88) | 25 (81) | 121 (82) |
| Currently pregnant | 2 (3) | 0 | 0 | 2 (1) |
| Country of origin | ||||
| Norway | 96 (84) | 45 (82) | 29 (83) | 170 (83) |
| Other countries | 19 (16) | 10 (18) | 6 (17) | 35 (17) |
| Age b | 31 ± 9 (18–56) | 30 ± 10 (18–60) | 28 ± 8 (20–52) | 30 ± 9 (18–60) |
| Body mass index, kg/m2 b | 23 ± 3 (17–33) | 24 ± 4 (18–40) | 23 ± 3 (18–32) | 23 ± 3 (17–40) |
| Educational level | ||||
| <12 years | 3 (3) | 1 (2) | 2 (6) | 6 (3) |
| 12 years | 22 (19) | 11 (20) | 3 (9) | 36 (18) |
| 1–4 years university | 90 (78) | 43 (78) | 30 (86) | 163 (80) |
| Smoking status | ||||
| No | 103 (89) | 49 (89) | 33 (94) | 185 (90) |
| Yes | 12 (11) | 6 (11) | 2 (6) | 20 (10) |
| Duration of vegan/vegetarian diet (years) b | 4 ± 3 (0.11–10) | 6 ± 3 (0.11–10) | 5 ± 4 (0.11–10) | 5 ± 3 (0.11–10) |
| Iodine supplement use, 24-h | ||||
| Yes | 57 (49) | 25 (45) | 18 (51) | 100 (49) |
| No | 58 (51) | 30 (55) | 17 (49) | 105 (51) |
| Iodine supplement use, habitually | ||||
| Yes | 69 (60) | 26 (47) | 10 (29) | 105 (51) |
| No | 46 (40) | 29 (53) | 25 (71) | 100 (49) |
| Consumption of macroalgae habitually | ||||
| Yes | 23 (20) | 8 (15) | 4 (11) | 35 (17) |
| No | 92 (80) | 47 (85) | 31 (89) | 170 (83) |
| Vegan a | n | Vegetarian a | n | Pescatarian a | n | p-Value b | ||
|---|---|---|---|---|---|---|---|---|
| 24-h intake | Food only | 19 (12, 30) | 115 | 17 (12, 30) | 55 | 16 (12, 29) | 35 | 0.732 |
| Supplements | 150 (150, 225) | 57 | 150 (150, 150) | 25 | 150 (150, 206) | 18 | 0.723 | |
| Total intake c | 92 (19, 171) | 115 | 70 (17, 165) | 55 | 123 (16, 176) | 35 | 0.720 | |
| Habitual intake | Food only | 16 (11, 21) | 115 | 16 (11, 23) | 55 | 20 (15, 30) | 35 | 0.037 * |
| Supplements | 150 (150, 150) | 69 | 150 (150, 150) | 26 | 150 (150, 225) | 10 | 0.061 | |
| Macroalgae | 865 (364, 1978) | 23 | 843 (705, 1590) | 8 | 375 (110, 610) | 4 | 0.091 | |
| Total intake c | 315 (19, 361) | 115 | 305 (15, 323) | 55 | 39 (16, 324) | 35 | 0.157 |
| Iodine Knowledge Score | Vegans (n = 111) n (%) | Vegetarians (n = 53) n (%) | Pescatarians (n = 31) n (%) | p-Value a | Total (n =195) n (%) |
|---|---|---|---|---|---|
| Very low (0–5 points) | 24 (22) | 14 (26) | 15 (48) | 53 (27) | |
| Low (6–11 points) | 55 (50) | 28 (53) | 14 (45) | 97 (50) | |
| Medium (12–19 points) | 32 (29) | 11 (21) | 2 (7) | 45 (23) | |
| High (20–26 points) | 0 | 0 | 0 | 0 | 0 |
| Mean score (± SD) | 8 ± 4 | 8 ± 4 | 5 ± 4 | 0.001 |
| Dependent Variable | Predictor Variables | Unadjusted Coefficient (CI 5 95%) | p-Value | Adjusted Coefficient 6 (CI 5 95%) | p-Value |
|---|---|---|---|---|---|
| UIC, µg/L 1 | |||||
| Vegan dietary practice 2 | −0.2 (−0.31, −0.04) | 0.01 | −0.2 (−0.16, −0.02) | 0.01 | |
| Iodine supplement use, last 24 h 3 | 0.2 (0.02, 0.29) | 0.02 | 0.2 (0.01, 0.15) | 0.03 | |
| Higher Education 4 | 0.2 (0.00, 0.34) | 0.01 | 0.1 (0.00, 0.14) | 0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Groufh-Jacobsen, S.; Hess, S.Y.; Aakre, I.; Folven Gjengedal, E.L.; Blandhoel Pettersen, K.; Henjum, S. Vegans, Vegetarians and Pescatarians Are at Risk of Iodine Deficiency in Norway. Nutrients 2020, 12, 3555. https://doi.org/10.3390/nu12113555
Groufh-Jacobsen S, Hess SY, Aakre I, Folven Gjengedal EL, Blandhoel Pettersen K, Henjum S. Vegans, Vegetarians and Pescatarians Are at Risk of Iodine Deficiency in Norway. Nutrients. 2020; 12(11):3555. https://doi.org/10.3390/nu12113555
Chicago/Turabian StyleGroufh-Jacobsen, Synne, Sonja Y. Hess, Inger Aakre, Elin Lovise Folven Gjengedal, Kristina Blandhoel Pettersen, and Sigrun Henjum. 2020. "Vegans, Vegetarians and Pescatarians Are at Risk of Iodine Deficiency in Norway" Nutrients 12, no. 11: 3555. https://doi.org/10.3390/nu12113555